It’s commonly believed, and portrayed in the media, that amnesia is nearly exclusively caused by physical damage to the structures of the brain. It is also likely that this is the main cause taught at GCSE level psychology, if not the only discussed cause.
While brain damage is arguably the most common of causes, such as in cases of WKS, however it’s not the only cause. In fact, one of the criteria to accurately diagnose TGA is the absence of evidence suggesting head injury/trauma (Hodges & Warlow, 1990). Where damage to brain structures is the cause however, it need not be a physical trauma, resulting from a car crash for example, but damage to structures as a result of a virus or prolonged substance abuse.
The currently accepted theory of WKS revolves around chronic alcoholism, paired with a poor dietary regime, leading to a thiamine (Vitamin B) deficiency. The poor dietary regime can cause Wernicke’s Encephalopathy (WE) which is an acute neuro-psychiatric condition caused by an inadequate supply of thiamine (vitamin B1) to the brain (Thomson, Guerrini, & Marshall, 2012). If left undiagnosed or not properly treated, WE can develop into WKS which is much more severe and is detailed in the previous ‘Signs/Symptoms’ section above.
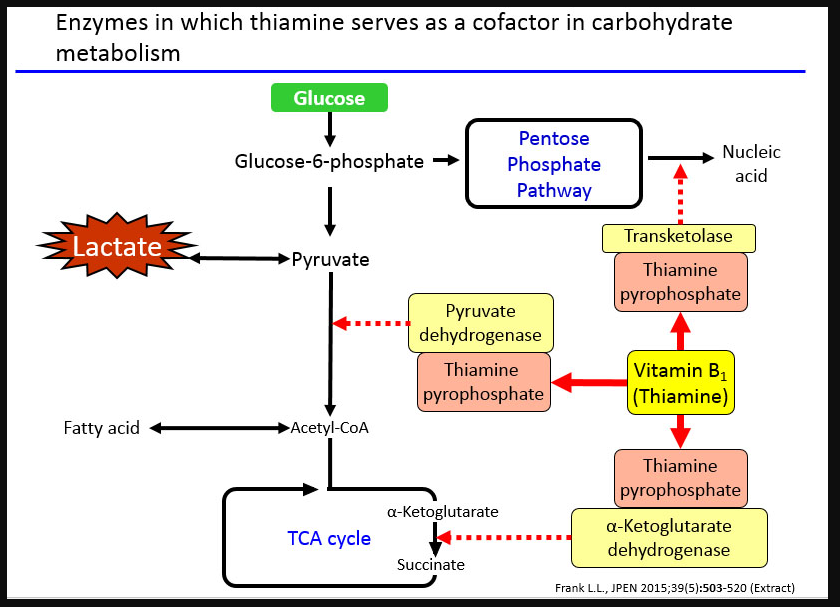
Thiamine is essential in the metabolism of glucose (the process is shown below in Figure 3) in the brain; the deficiency causes a loss, and/or shrinkage, of the neurons (Kalat, 2016). It has been noted the in WKS patients this loss/shrinkage of neurons often seems to be comprised of cholinergic neurons where the brain damage occurs in the basal forebrain (Nardone, et al., 2010).
However, the damage to the basal forebrain doesn’t explain the persistent amnesia in cases of WKS; there must be damage to other structures/areas. Malamud & Skillicorn (1956) suggested that it was lesions to the mammillary bodies (Figure 4) causing the amnesia, whereas Victor et al (1989) posed that it was in fact the Dorsomedial Thalamic Nuclei (DMTN) (Figure 5). More recent research has found that mammillary bodies or DMTN alone were insufficient to cause the amnesia associated with WKS; only if both had suffered damage did the amnesia occur (Zuccoli, et al., 2009).
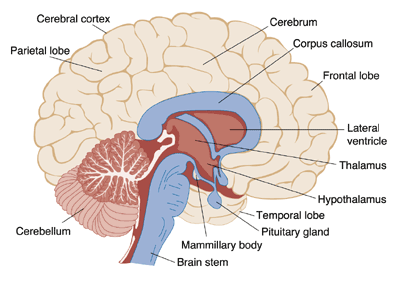
Figure 4. Identifying various brain structures (including Mammillary Bodies)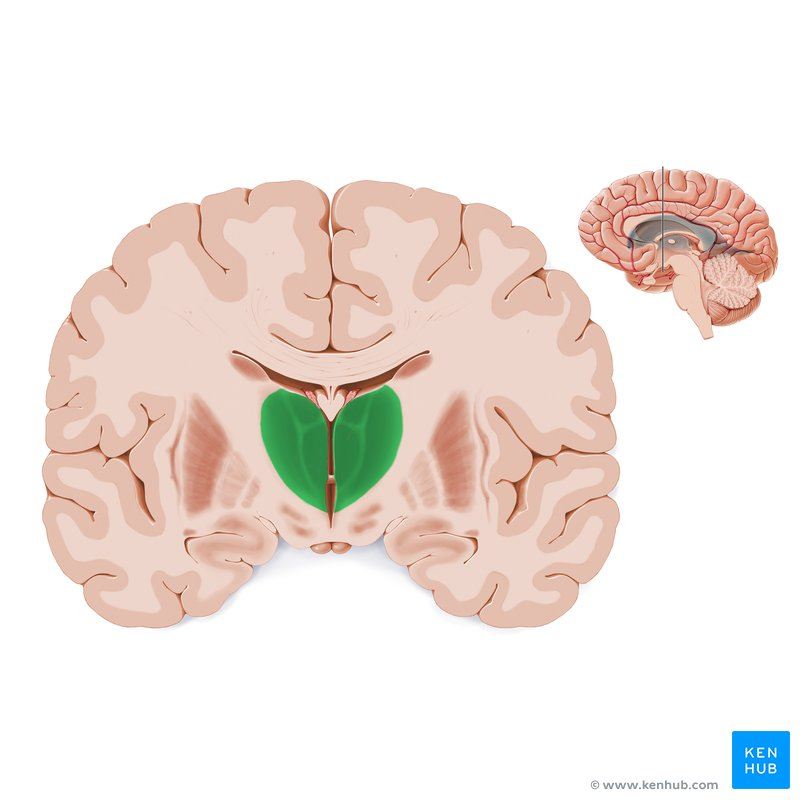
Figure 5. Highlighting location of Dorsomedial Thalamic Nuclei
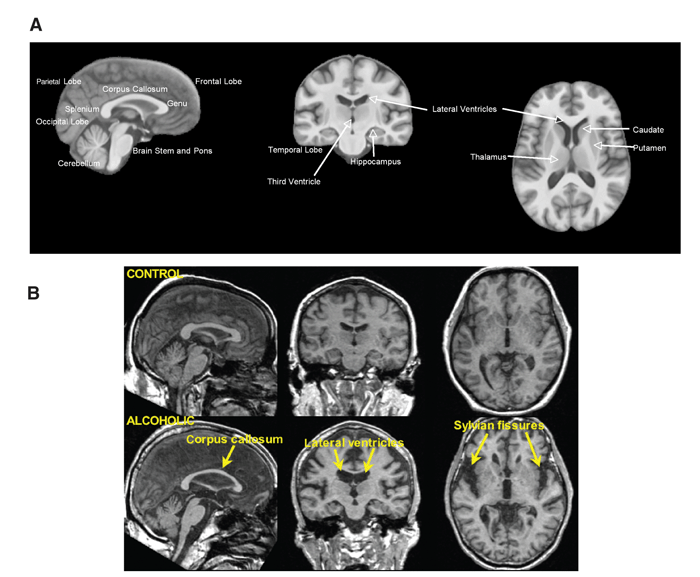
Similar research has found that 80% of patients had evidence of symmetrical lesions to the medial thalami and periventricular region of the third ventricle (Zuccoli, et al., 2009). Figure. 6 below identifies some of these brain structures (A), as well as how they differ in ‘alcoholic’ and ‘non-alcoholic’ participants (B).
It has been argued that issues with this explanation of WKS are that whilst poor diet and chronic alcohol abuse can quite reasonably contribute to a thiamine deficiency, it doesn’t explain the absence of WKS cases in famine situations where thiamine deficiencies are prevalent. Thomson, Guerrini & Marshall countered (2012) thiamine deficiency leads to a reduction in the activity of thiamine-dependent enzymes, and in turn to alterations in mitochondrial activity, impairment of cell metabolism, decreased energy status and eventually selective neuronal death. The damage caused by the combination of thiamine deficiency and alcohol metabolism probably interferes with adequate thiamine transport at a number of sites in the body, including the blood–brain barrier, as well as causing damage to the inactive thiamine-dependent enzymes which then require higher concentrations of thiamine to work normally.; however, the issue of why non-alcoholics are able to develop WKS remains.
For other disorders different individuals can be at a greater risk to develop them, for example key risk factors of TGA have been identified and include a history of migraines, ischemic heart disease (Also known as coronary heart disease, when insufficient oxygen reaches the heart muscle), carotid atheromasia (The presence of a atheroma blocking the carotid artery) and psychophysical stress (The effect of psychological stress on the physical body) (Jang, Park, & Hong, 2014) (Agosti, Akkawi, & Borroni, 2006).
TGA episodes are most likely to occur females and in the 7th decade of life (with a mean age of 61-67.3 years), supposedly due to the fact risk factors and naturally associated pathologies have a higher rate of incidence (Arena, Brown, & Mandrekar, 2017).
Whilst the above risk factors have been suggested to increase the likelihood of a TGA episode, it has also been found that ‘close’ and ‘remote’ precipitating events can be triggers leading to an episode. Close precipitating events for TGA include emotional stress, physical effort/exertion (this includes sexual activity and orgasms (Lane, 1997)) and water contact/extreme temperature change; whereas remote precipitating events would include anxiety (particularly a work/home conflict), general health problems and even financial stressors (Erkelens & Snoek, 2010).
Research has also indicated to some specific biological causes of TGA. Such as a stress-induced catecholamine release may lead to hypoxia/ischaemia, or neurotransmitters involved in this release may affect the formation of memories (Finsterer & Stöllberger, 2017). Alternatively, Spiegel, McCroskey & Deyerle (2016) found that severe emotional stress may contribute to the destabilisation of the CA1 sector of the Hippocampus via a massive glutamate release; leading to a disruption in the formation of memories.
On the other hand, TGA episodes may also be considered a psychological defensive mechanism, in cases of psychological disorders such as PTSD and dissociative disorders, associated to a phobic personality trait (Portaro, et al., 2018). Furthermore, psychological stressors, a psychogenic cause, appeared to disturb the affective learning circuit between the amygdale, hippocampus, striatum and the prefrontal cortex. As well as affecting the inhibiting effects on the amygdala; disrupting the memory formation process (Spiegel, McCroskey, & Deyerle, 2016). It is important to consider both biological and psychological causes for the TGA as they are both prominent factors in cases; 90% of examined TGA episodes involved physical or psychological precipitating factors (Quinette, et al., 2006).
